medicine online blended assignment
Medicine blended assignment
Name: k.shirisha
rollno: 60
I have been given the following cases to solve in an attempt to understand the topic of \"patient clinical data analysis \"to develop my competency in reading and comprehending clinical data including history,clinical findings,investigations and diagnosis and come up with a treatment plan
This is the link of the questions asked regarding the cases
http://medicinedepartment.blogspot.com/2021/05/online-blended-bimonthly-assignment.html?m=1
Below are my answers to the medicine assignment based on my comprehension of the cases
First case:
Pulmonology;
A 55 year old female with" shortness of breath,pedal edema and facial puffiness
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
Questions:
1)What is the evolution of the symptomatology in this patient in terms of an event time line and wher is the anatomical localization for the problem and what is primary etiology of the patients problem.
Ans: Symptomatology:
The patient has following features:
* shortness of breath since 20 years ( on and off) lasted for 1 week and relieved on medication
latest episode of her sob started 30 days ago which was grade 4
*pedal edema: upto the level ankle
Type: pitting since 15 days
* facial puffiness: since 15 days
* she is known case of diabetes since 8years
* Hypertension is diagnosed 20 days ago treated for the same
* 5 years ago she was treated for anemia with iron injections
on 30/4/2021 she had sputum examination which was negative for Afb.on 4/5/2021 she was started on empirical ATT. this resulted in generalized weakness.a few days after ATT she started developing pedal edema and facial puffiness.
The ATT was stopped 16/5/21 on advice of pulmonologist
drowsiness since 2 days
decreased urine out put since 2 days
Surgical history:
Operated for intestinal perforation 20 years ago
Om investigations:
HRCT imaging: signet ring sign
Anatomical localisation for problem;
Lungs bronchial tube
Primary etiological agent:
* Biomass combustion with poor ventilation used for cooking
2) what are MOA,indication and efficacy are placebo of each of pharmacological and non pharmacological interventions used for this patient
Ans;
Pharmacological interventions:
1) injection Augmentin:(amoxycillin,clavulinic acid potassium).
MOA; Amoxicillin- binds to penicillin binding proteins within in the bacterial cell wall and inhibits cell wall synthesis
clavulinic acid:
B lactam structurally related to penicillin,that may inactivate certain Blactamase enzymes
indications:
copd, lower respiratory tract infections
efficacy: 87.2%
placebo
2)
Tab: azithromycin 500mg
moa:
Azithromycin binds to the 23S rRNA of the bacterial 50S ribosomal subunit. It stops bacterial protein synthesis by inhibiting the transpeptidation/translocation step of protein synthesis and by inhibiting the assembly of the 50S ribosomal subunit
indication: respiratory tract infections
efficacy; 82.9%
3)inj lasix:
moa:
Furosemide, like other loop diuretics, acts by inhibiting the luminal Na-K-Cl cotransporter in the thick ascending limb of the loop of Henle, by binding to the chloride transport channel, thus causing sodium, chloride, and potassium loss in urine.
indication: heart failure
efficacy:
4)Tab: pantop40mg po od,
moa:

indication: For heartburn and chest pain due to stomach acid reflux disease in which acidic content from stomach comes up to food pipe and mouth.
efficacy:
5) inj hydrocortisone100mg iv:
moa: Hydrocortisone binds to the glucocorticoid receptor leading to downstream effects such as inhibition of phospholipase A2, NF-kappa B, other inflammatory transcription factors, and the promotion of anti-inflammatory genes.
indication: Anti infammatory effect;
Acute exacerbation of COPD
efficacy:
6) neb with ipravent,budecort 6hourly
7) pulmoclear 100mg po od
Moa;
Pulmoclear works by relaxing the airways and loosening the cough, thus making the expulsion of cough easy.
Pulmoclear Tablet is used for relieving the symptoms of coughing, wheezing, congestion and blockage in the airways in a condition called chronic obstructive pulmonary disease (COPD).09-Apr-2021
8)injHAISc(8am-2pm-8pm)
It works by helping move sugar from the blood into other body tissues where it is used for energy. It also stops the liver from producing more sugar. All of the types of insulin that are available work in this way
9) inj Thiamine 1amp in 100ml of ns:
Non pharmacological interventions:
Head end elevation
O2 inhalation to maintain spo2 above 92%
Intermittent Bipap for 2hrs
Chest physiotherapy
Grbs 6th hrly
Temp,bp,pr,spo2monitering
I/O charting
3)What could be causes for her current acute exacerbation?
ans:

In this patient current exacerbation is bronchiectasis,heart failure
4. Could the ATT have affected her symptoms? If so how?
Ans
5.What could be the causes for her electrolyte imbalance?
Ans
Bronchiectasis, heart failure , copd
2) second case:
Neurology;
A) 40 year old male presented to old with chief complaints of irrevalent talking and decreased food intake since 9 days
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans: symptomatology;
Irrevalent talking, decreased food intake 9days
Laughing himself,
He was chronic alcoholic since 12 years
Previously, he had 2-3 episodes of seizures, one being 1 year ago and the most recent being 4 months ago. The most recent time, (4 months ago), he had developed seizures (most probably GTCS) following cessation of alcohol for 24 hours, which was associated with restlessness, sweating, and tremors. Following this episode, he started drinking again.
He is known case of diabetic
He also had short term memory loss since 9 days, where he could not recognize family members from time to time.
2x2cm chronic ulcer on heel of R foot with sloping edges
Investigtions
Smear findings: Normocytic normochromic anemia, leukocytosis
Serum electrolytes
Albumin: 3.3g/dL (decreased
RFT
9.RBS
2D ECHO
-Mild LV hypertrophy
USG abdomen
-Bilateral Grade1 RPD
-Echogenic intramural foci noted in gallbladder
Anatomical localisation; brain, kidneys , foot ulcer on right leg
Primary etiological agent: chronic alcohol abuse
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans:IVF NS and RL @150ml/hr
3) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier? What could be a possible cause for this?
Ans: Because these symptoms are not due to alcohol withdrawal.
Possible cause is uremic encephalopathy due to excessive toxins that are accumulated in brain caused encephalopathy signs
4) What is the reason for giving thiamine in this patient?
It is a B1 supplement used to treat thiamine deficiency
In chronic alcoholic s there will be deficiency of thiamine and also to treat ecephalopathy wernickes
5) What is the probable reason for kidney injury in this patient?
Ans:diabetes
Azotemia_ increased urea levels ,creatinine levels increased , hyperuricemia,
6). What is the probable cause for the normocytic anemia?
Ans: increased blood loss
Chronic kidney diseaae
7) Could chronic alcoholism have aggravated the foot ulcer formation? If yes, how and why?
Ans: no,it is an diabetic foot open wound ulcer
Heals slowly , individuals with diabetes have poor circulation of blood
People with diabetes have slow healing process and heals slowly
B)A 52 year old male with cerebellar ataxia
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
Questions;
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Symptomatology; slurring of speech, deviation of mouth since 2 days and
Giddiness associated with Bilateral Hearing loss, aural fullness and presence of tinnitus.
vomiting- 2-3 episodes per day, non projectile, non bilious containing food particles.
H/o postural instability- he is unable to walk without presence of supports, swaying is present and he has tendency to fall while walking
Medical History- Patient was found to have denovo HTN, and he did not continue taking medication regularly.
He is a chronic alcoholic, been consuming alcohol since 30 years, consumes 90-180 ml daily
Ataxic gait
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Tab Veratin 8 mg PO TID; it is a antihistamine ( betahisine)
MOA;
Betahistine has two mechanisms of action. Primarily, it is a weak agonist on the H1 receptors located on blood vessels in the inner ear. This gives rise to local vasodilation
and increased permeability, which helps to reverse the underlying problem of endolymphatic hydrops.
Indication ; meniere's disease
Inj Zofer 4 mg IV/TID

Indication ; vomiting
Tab Ecosprin 75 mg PO/OD

Indication: anti-inflammatory, infracts
Tab Atorvostatin 40 mg PO/HS

Indication ; used to lower high blood pressure to treat strokes,lowers cholesterol synthesis
BP monitoring- 4rth hourly
Tab Clopidogrel 75 mg PO/OD
Anti patelet

Inj Thiamine 1 AMP in 100 ml NSPO/BD
MOA;

3) Did the patients history of denovo HTN contribute to his current condition?
Yes
4) Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic type of stroke?
Hypertension
C) A 45 years old female ,house wife by occupation came to opd with chief complaints of palpitations,chest heaviness,pedal edema,chest pain,radiating pain along her left upper limb
http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
Questions:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Palpitations since 5 days
Pain along her left upper limb associated with tingling and numbness-6 days
*Chestpain -since5 days
*Difficulty in breathing-5 days
*Swelling over the legs(bilateral)-8 months
bilateral pedal edema which is gradually progressing and it is present both in sitting and standing position and relieved on taking medication.
Palpitations: since 5days which are sudden in onset,more during night time and aggregated by lifting weights, speaking continuously and it is relieved by drinking more water, medication
*dyspnoea during palpitations (NYHA-CLASS-3)-since5 days
*Pain:since 6days radiating along the left upper limb which is dragging in nature, aggrevated during palpitations and relieved by taking medication for palpitations.
*Chest pain associated with chest heaviness
right and left)paresis due to hypokalemia 1year back
2 months back came to KIMS NARKETPALLY for treatment of neck pain for which she received medication:
10 yrs back had the episode of paralysis of both upper and lowerlimbs(rt and left)
2) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Cervical spondylosis, due to intrinsic muscle wasting Hypokalemia occurs
Risk factors;
Cervical spondylosis
Paresis
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
Disappearance T wave
Progressive increase in amplitude of u wave
First and second degree AV
ST segment depression
Symptoms; palpitations, chest pain, neck pain, bilateral pedal edema pitting type
D) 55years old patient with seizures.
Questions;
1. Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
Yes,

2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Ans; Because it get severed on left side onlyBut in recent it get severed all over the body
This disturbance is caused by electrical signals spreading through the brain inappropriately. Often this will result in signals being sent to your muscles, nerves, or glands. The spread of these signals in your brain can make you lose consciousness and have severe muscle contractions
Abnormal increased activity in fronto-parietal association cortex and related subcortical structures is associated with loss of consciousness in generalized seizures.
E)
A 48 year old male with seizures and altered sensorium
Questions;
Questions: 1) What could have been the reason for this patient to develop ataxia in the past 1 year?
Minor head injury or neurological deficit
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
Head trauma,alcoholism
Seizures contribute to bleeding diathesis
F) A 30 YR OLD MALE PATIENT WITH WEAKNESS OF RIGHT UPPER LIMB AND LOWERLIMB
Questions
1.Does the patient's history of road traffic accident have any role in his present condition?
Yes
2.What are warning signs of CVA?
Ans;. There may be no warning signs of stroke until it occurs
It is why high blood pressure one of risk factors for stroke - silent killer
3.What is the drug rationale in CVA?

4. Does alcohol has any role in his attack?
Yes
5.Does his lipid profile has any role for his attack??
Yes
G)
A 50 YEAR OLD PATIENT WITH CERVICAL MYELOPATHY
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
Questions:
1)What is myelopathy hand ?
There is loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and release rapidly with these fingers. These changes have been termed myelopathy hand

2)What is finger escape ?
- Described by Ono as a one of the signs in cervical cord damage
- Deficient adduction and or extension of the ulnar 2-3 digits
- Differentiating it from other similar looking signs affecting the little finger
3)What is Hoffman’s reflex?


H) A 17 year old female with seizures
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
Questions:
1) What can be the cause of her condition ? Metabolic causes; hypokalemia
Systemic; dehydration
2) What are the risk factors for cortical vein thrombosis?
Iron deficiency anemia
Dehydration
Seizures( focal or generalized)
Headache
3)There was seizure free period in between but again sudden episode of GTCS why?resolved spontaneously why?
4) What drug was used in suspicion of cortical venous sinus thrombosis?
Treat infection with antibiotics
Anticoagulants are indicated( low molecular weight heparin orUFH)
Adequate dehydration
Antiedema measures if needed

3) Cardiology (10 Marks)
A)
A 78YEAR OLD MALE WITH SHORTNESS OF BREATH, CHEST PAIN, B/L PEDAL EDEMA AND FACIAL PUFFINESS
Questions;
1.What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction?
- Preserved ejection fraction (HFpEF) – also referred to as diastolic heart failure. The heart muscle contracts normally but the ventricles do not relax as they should during ventricular filling (or when the ventricles relax).
- Reduced ejection fraction (HFrEF) – also referred to as systolic heart failure. The heart muscle does not contract effectively, and therefore less oxygen-rich blood is pumped out to the body.
2.Why haven't we done pericardiocenetis in this pateint?
It is resolving with antibiotics or it cause ruputre to lungs
3.What are the risk factors for development of heart failure in the patient?
Ans:
Age, hypertension, obesity, diabetes
4.What could be the cause for hypotension in this patient?
Pericardial effusion
Acute pericarditis
B)
A 73 YEAR OLD MALE PATIENT WITH PEDAL EDEMA, SHORTNESS OF BREATH AND DECREASED URINE OUTPUT
Questions;
1.What are the possible causes for heart failure in this patient?
Obesity, hypertension, Diabetes, chronic kidney disease

2.what is the reason for anaemia in this case?
Chronic kidney disease
Heart failure with preserved ejection fraction
Diabetic retinopathy
Hypoxia-
3.What is the reason for blebs and non healing ulcer in the legs of this patient?
Reason for bleb infection by environmental agents or organisms
Prolonged pressure on feet,circulatory problems
Kidney failure
Diabetes
High cholesterol
High blood pressure
These conditions impair the circulation and damages nerves leads to non healing ulcer
4. What sequence of stages of diabetes has been noted in this patient?
sequence of stages of diabete s in this patient are diabetes are insulin resistance, prediabetes, type 2 diabetes and type 2 diabetes and vascular complications, including retinopathy, nephropathy or neuropathy and, or, related microvascular events.
C)Atrial fibrillation and bilateral thrombus in a 52 year old male
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
Questions
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
decreased urine output and shortness of breath at rest since one day.
- Shortness of breath Grade II (on exertion) which progressed to Grade IV (at rest) for which he visited local RMP and was referred to our hospital.
- Patient also complains of decreased urine output since 2 days and Anuria since morning.
- CBP;
* Hemoglobin - 12.8 gm/dl
* Neutrophils - 87%
* Platelets - 88000
Renal function test
* Urea - 198mg/dl
* Creatinine - 5.4mg/dl
* Uric acid - 11.9mg/dl
* Phosphorus - 5.6mg
Blood Urea - 122mg/
* Serum Creatinine - 3.2mg/dl
Liver function test
* Total Bilirubin - 2.96mg/dl
* Direct Bilirubin - 1.93mg/dl
* SGOT - 476 IU/L
* SGPT - 551 IU/L
* Alkaline Phosphate - 172 IU/L
CT pulmonary angiogram
* Dilated Main Pulmonary Artery and Left Pulmonary Arteries.
* No evidence of Pulmonary Arterial Embolism.
*Thrombi noted in Left Atrial Appendages and Left atrium
9. 2D Echo
* Dilated All chambers
* Global Hypokinesia
* Severe LV dysfunction (EF = 28) (Moderate to severe eccentric TRF positive)
* IVC dilated 2.15 cms
Anatomical localisation ; heart, lungs
Primary etiologic agent; chronic alcoholic, hypertension diabetes
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Pharmacological interventions;
the day of admission -
* INJ. Dobutamine 3.6ml/hr was given to maintain the falling BP up to a MAP of 55 mmHg.

On Day 3 -
* ECG showed Irregular rhythm and he was started on TAB. Digoxin 0.25mg OD 5/7 and INJ. Unfractionated Heparin 5000 IU TID.
* As patient's D DIMER was high, Anti coagulants were started and planned for CPTA.
On Day 4 -
* Patient was started on TAB. Carvediol 3.125mg BD
On Day 5 -
* Patient's Serum Creatinine and Serum Urea were increased after CPTA.
* Nephrology opinion was taken in view of Contrast Induced Nephropathy.
On Day 6 -
* Patient was started on INJ. Unfractionated Heparin Infusion @5ml/hr and TAB. Acetyl cysteine 600mg PO TID.
* Daily monitoring of APTT, PT, INR and RFT was done.
On Day 7 -
* TAB. Acitrom 2mg OD was started.
On Day 8 -
* The Infusion of Heparin was increased to 7ml/hr and it was stopped after attaining the APTT of >70secs, PT of 23secs and INR of 2.3.
Other medications used during the course in hospital -
1. TAB. Cardivas3.125mg PO/BD
Moa
Carvedilol reversibly binds to beta adrenergic receptors on cardiac myocytes. Inhibition of these receptors prevents a response to the sympathetic nervous system, leading to decreased heart rate and contractility.
Indication; CCF,left ventricular dysfunction, high blood pressure
2. TAB. Dytor 10mg PO/OD
Dytor 10 Tablet works by increasing the amount of urine produced. This helps your body get rid of extra water thereby relieving symptoms such as shortness of breath and swelling in your arms, legs, or abdomen. This will help you go about your daily activities more easily and make you more confident about being active.
Indication; treats high blood pressure, excessive accumulation of water in body
3. TAB Pan D 40mg PO/OD

4. TAB. Taxim 200mg PO/OD
Taxim Injection works by inhibiting the formation and growth of bacterial cell wall which eventually leads to the death of the bacteria responsible for causing infection
5. INJ. Thiamine 100mg in 50ml NS IV/TID
6. INJ. HAI S.C 8U-8U-6U
Used to control blood sugar levels
3) What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?

Type-4 cardiorenal syndrome
4) What are the risk factors for atherosclerosis in this patient?
Hypertension, CCF ,left ventricular dysfunction,
Diabetes ,old age
5) Why was the patient asked to get those APTT, INR tests for review?
ApTT - To check time at which clots are formed
INR- To moniter blood thinning medication
D)
67 year old patient with acute coronary syndrome
Questions
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
shortness of breath (SOB) since 1/2 hour.
She had H/O heartburn like episodes since a year. They were relived without use of any medication.
She has H/O TB diagnosed 7 months ago for which she completed the course of medication a month ago.
Patient was apparently asymptomatic till 9pm on that day (27/4/21). She apparently ate dinner and slept. When she woke up at night for washroom she developed sweating on exertion and shortness of breath even at rest.
K/C/O of DM2 since 12 years and is on Rx GLIMI M2 PO/BD
K/C/O of hypertension since 6 months and is on Rx TELMA 20 mg PO/OD
H/O pulmonary TB 7 months ago when she had cough, chest pain. Completed the course for TB a month ago. Currently negative for TB.
INVESTIGATIONS-
1) An ECG was done upon admission. The ECG shows NSTEMI ( acute coronary syndrome)
ECG will show the following characteristics for an NSTEMI:
- depressed ST wave or T-wave inversion
- no progression to Q wave
- partial blockage of the coronary
Anatomical localisation ; heart, coronary arteries
Primry etiological agent;
Causes:
- Atherosclerosis – Also known as coronary artery disease, this condition is the most common cause of heart attacks and occurs when the buildup of fat, cholesterol, and other substances forms plaque on the walls of the coronary arteries
- Coronary artery spasm – A rare cause of blockage, spasms of the coronary arteries can cause them to become temporarily constricted.
- Coronary artery tear – Also known as a spontaneous coronary artery dissection, a tear in a coronary artery can prevent blood from reaching the heart and cause a heart attack.
- High cholesterol
- Hypertension
- Smoking
- Illicit drug abuse
- Obesity
- Stress
- Type 1 DM
- Family history
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Upon seeing the ECG, the patient was given TAB MET XL 25 MG/STAT.
Met XL 25 tablet works by relaxing the blood vessels, slowing down the heart rate. By doing this, it reduces the workload on the heart of pumping the blood effectively
Non pharmacological interventions ; per cutaneous intervention
Indication; used to treat high blood pressure mainly, along with certain heart conditions such as angina (chest pain) and heart failure. Decreased blood pressure helps prevent other conditions like kidney problems, stroke, heart attack and migraine
3) What are the indications and contraindications for PCI?
4) What happens if a PCI is performed in a patient who does not need it? What are the harms of overtreatment and why is research on overtesting and overtreatment important to current healthcare systems?
Common complications of pci;
Hematoma, bleeding ,pseudoaneurysm at access site
Absolute Contraindications:
- Noncompliance with the procedure and inability to take dual antiplatelet therapy.
- High bleeding risk (thrombocytopenia, peptic ulcer, severe coagulopathy)
- Multiple percutaneous coronary intervention restenosis
Relative Contraindications:
- Intolerance for oral antiplatelets long-term
- Absence of cardiac surgery backup
- Hypercoagulable state
- High-grade chronic kidney disease
- Chronic total occlusion of SVG
- An artery with a diameter of <1.5 mm
- Stenosis of <50%
cardiac arrest (4.1%), death (4.1%), stroke (1%), shock (9.8%), respiratory failure (6.4%) and high-grade atrioventricular block requiring treatment (4.6%).
So overtreatment is important in current health care system.
E) A 60year old Male patient, resident of xxxxxxxx, came to the OPD with the Chief complaint of chest pain since 3 days and giddiness and profuse sweating since morning
GRBS: 626mg/dl
On evaluation his GRBS was very high. He was immediately given 6U oh HAI iv and then his GRBS was checked which showed 506mg/dl so he was administered 16U of Actrapid
INTERPRETATION: increased urea, creatinine, uric acid and hyponatremia.
Causes:
- Atherosclerosis – Also known as coronary artery disease, this condition is the most common cause of heart attacks and occurs when the buildup of fat, cholesterol, and other substances forms plaque on the walls of the coronary arteries
- Coronary artery spasm – A rare cause of blockage, spasms of the coronary arteries can cause them to become temporarily constricted.
- Coronary artery tear – Also known as a spontaneous coronary artery dissection, a tear in a coronary artery can prevent blood from reaching the heart and cause a heart attack.
- High cholesterol
- Hypertension
- Smoking
- Illicit drug abuse
- Obesity
- Stress
- Type 1 DM
- Family history

TAB ATORVAS 80mg PO/STAT

Indication ; To lower cholesterol synthesis, high blood pressure
TAB CLOPIBB 300mg PO/STAT
It is an antiplatelet medicine or blood thinner helps to prevent formation of blood in your blood vessels
This helps to lower the chances of you getting heart attack or stroke
It is widely used medicine for heart protection
INJ HAI 6U/IV STAT
Used to correct blood glucose levels
Blood pressure monitoring

A 33 YEAR OLD MAN WITH PANCREATITIS, PSEUDOCYST AND LEFT BRONCHO-PLEURAL FISTULA
Abdominal pain was incresed after food intake.
* Pain is throbbing type and radiating to back and is associated with nausea and vomiting( 1 episode) , which is non bilious, non projectile and also has food particles and water content 1 week.
* Fever was high grade, continuous and associated with chills and rigors.
Then he developed constipation since 4 days and passing flatus.
* patient also had burning micturition since 4 days, which is associated with suprapubic pain, increased frequency and urgency
* No history of blood or mucus in stools.
* No other complaints.
khaini : 1 per day since 5 yrs.
3) Ghutka: 5 per day since 6 months
Tenderness present over umbilical, left hypochondriac, left lumbar, hypogastric and suprapubic region.
* Guarding and rigidity : present
1) CE CT ( Contrast Enhanced CT):
* Showing pseudocyst and infective fluid collections
2)Chest x ray:
* 1 st image showing pleural effusion and basal atelectasis and 2 nd image shows pneumothorax ( collapsed lung ) which developed in the course of hospital.CBP showed LEUCOCYTOSIS.
* LFT showed Increased ALP and decreased ALBUMIN.
* Pleural fluid was EXUDATIVE in nature according to lights criteria and pleural fluid amylase being: 469 mg/dl.
* CE CT abdomen shows ; LARGE PSEUDOCYST COMPRESSING STOMACH (Dimensions: 15*9*10 cms ) & MULTIPLE INFECTIVE FLUID COLLECTION IN MIDLINE ALONG ANTERIOR ABDOMINAL WALL AND SUB HEPATIC REGION; WHICH ARE CONTINUOUS AND LOCULATED ASCITIS.
Chest x ray showed; MODERATE PLEURAL EFFUSION , BASAL ATELECTASIS IN LEFT LUNG
LEFT PNEUMOTHORAX SECONDARY TO BRONCHO PULMONARY FISTULA
1) ING. MEROPENAM ; TID for 7 days
Meropenam broad spectrum antibiotic used to treat abdominal infections caused by bacteria
cure rates with meropenem were 86.2% and 73.1%,
2) ING. METROGYL 500 mg IV TID for 5 days
Inj metrogyl ha metronidazole an antibiotic
Metronidazole is effective for the management of anaerobic infections, such as intra-abdominal infections, respiratory tract infections
3) ING. AMIKACIN 500 mg IV BD for 5days
Aminoglycoside antibiotic used to treat intra abdominal ,lung infections
## Here all three of these (Inj. Meropenem, Inj. Metrogyl, Inj. Amikacin ) are used as antibiotics to control infection and ; to prevent septic complications of acute pancreatitis.
4) TPN ( Total Parenteral Nutrition )
* Method of feeding that by passes gastrointestinal tract
* Fluids are given to vein , it provides most of the nutrients body needs.
* TPN has proteins, carbohydrates, fats, vitamins, minerals.
5) IV NS / RL at the rate 12l ml per
Given for fluid replacement ie., treat dehydration
6) ING. OCTREOTIDE 100 mg SC , BD
It is a Somatostatin long acting analogue.
* It is used here to decrease exocrine secretion of pancreas and it also has anti- inflammatory & cytoprotective effects.
7) ING. PANTOP 40 mg IV , OD
Inj. Pantop has PANTOPRAZOLE ( Proton Pump Inhibitor) used for its anti pancreatic secretory effect.
8) ING. THIAMINE 100 mg in 100 ml NS IV , TID
It is B1 supplement.
* It is given here because; due to long fasting & TPN usage , body may develop B1 deficiency
* Wernicke encephalopathy secondary to B1 deficiency may be caused... so a prophylactic B1 supplemention is necessary
9) ING. TRAMADOL in 100 ml NS IV , OD
* It is an opioid analgesic, given to releive pain
## After 4 days of this treatment; there is no improvement in patient and infact he is deteriorating clinically !!!
A 45 year old Female patient with Fever, Pain abdomen, Decreased Urine output and Abdominal distension
Post TURP
with non oliguria ATN
Diabetic Nephropathy
An Eight year old with Frequent Urination
A 40 YEAR OLD LADY WITH DYSPHAGIA, FEVER AND COUGH






LIVER ABSCESS
2. Amoebic Liver Abscess and Alcohol
A close relationship between the consumption of indigenously brewed alcohol beverages and the occurrence of ALA in the tropics has been established over a period of time by several large-population studies [3, 4, 5]
Reasons for this association between local alcohol beverages and ALA could be multifactorial. Factors influencing the association could be related to the pathogen, contents of beverages, status of the liver, and the immunity of the host. They are more vulnerable perhaps due to the large infective dose of Entamoeba histolytica and other bacterial pathogens ingested with the unhygienically brewed beverage. Associated nutritional status of the population and poor sanitation could also play a pivotal role. Hai et al. stated that alcohol-induced hepatic dysfunction and possible suppression of amoebistatic immune mechanisms by substances in the beverages could also be attributed in the mechanism [6].
Mukhopadhyay et al. [5] have suggested that “alcohol can predispose to ALA through a multitude of mechanisms, including hepatic damage by alcohol, lowered body resistance and suppression of liver function due to poor nutritional status of habitual consumers of alcohol, increased presence of amoebae in the liquor prepared locally with poor regard to aseptic procedures, and depression of immune mechanisms in chronic alcoholics.” A study conducted in India in 2011 [4] showed that 67.5% of patients with amoebic liver abscess are from the low socioeconomic class and 72% were alcoholics. It was also noted that alcoholics had larger abscesses, a greater frequency of complications, and delayed resolution of the abscesses.

INDICATIONS OF LIVER ABCESS DRAINAGE:
1) If the abcess is large ( 5cm or more) because it has more chances to rupture.
2) If the abcess is present in left lobe as it may increase the chance of peritoneal leak and pericardial leak.
3) If the abcess is not responding to the drugs for 7 or more days
Method of abcess drainage:* Aspiration using needle or catheter under imaging
50/Male came with altered sensorium


- Invited Mini Review
- Published:
Fungal Rhinosinusitis: Unravelling the Disease Spectrum
Journal of Maxillofacial and Oral Surgery volume 18, pages164–179 (2019)
Abstract
Fungal rhinosinusitis (FRS), once considered a rare disease, has seen a steep rise in incidence in recent times. This global rise in the burden of fungal disease is a consequence of an increment in the population with weakened immune systems. Increased life expectancy with rise in conditions like diabetes mellitus, medical advancements with invasive interventions, use of immunosuppressive drugs and chemo-radiotherapy all lead to unique risk situations. The situation becomes more alarming with the fact that there has been a significant rise in cases in immune-competent hosts with no predisposing factors. FRS represents a wide spectrum of disease ranging from the mild form of superficial colonization, allergic manifestations to life threatening extensive invasive disease. The categorization of disease into acute and chronic and invasive or noninvasive is important factor with implications in disease management and prognosis and this has been emphasized greatly in recent years. Diagnosis of FRS has been a challenge as the presenting clinical signs and symptoms and radiographic manifestations are often nonspecific. Definitive diagnosis requires direct fungi identification and hence culture and microscopic examination remain the gold standard. Availability of advanced and rapid diagnostic techniques is rare in majority of developing nations. Therapeutic dilemmas are another aspect of the management of FRS as in spite of the availability of new antifungal drugs, treatment is often empirical due to non-availability of early diagnosis, rapid disease progression and high costs of antifungal drugs. A description of the different types of FRS, their diagnosis and management has been presented in this review
Key words; fungal rhinosinuitis, mucormycosis, invasive fungal sinusitis
Covid pneumonia in a pre existing case of interstitial lung disease
The triggering of post-COVID-19 autoimmunity phenomena could be associated with both transient immunosuppression and an inappropriate form of immune reconstitution in susceptible individuals
A 50 year old female with Viral Pneumonia secondary to Covid-19

A 26 Year Old Female with Fever and Shortness of Breath
Ventilator Effectiveness
Outcomes can vary according to medical circumstances, but historical data provide some insight. The most comprehensive evaluation of prolonged (generally >14 days) mechanical ventilation is a 2015 meta-analysis of 124 observational studies, which found that 57% of patients suffering from various conditions were liberated from mechanical ventilation and 38% were alive at 1 year.
29 year old male patient with viral pneumonia secondary to COVID-19

45 Y/O MALE WITH COVID-19 AND COMORBIDITIES (ALTERED SENSORIUM, AZOTEMIA, HYPOKALEMIA.)
65 YEARS OLD MALE WITH VIRAL PNEUMONIA SECONDARY TO COVID-19.

A 67 year old lady in the ICU with COVID induced Viral Pneumonia .
What precautions should a recently-recovered COVID-19 patient take? Find out
'After the acute phase of COVID-19 is over, patients may return to hospitals with symptoms such as lethargy, body aches and itchy throats, even four to six weeks later,' says Dr Md Shakeel of Hiranandani Hospital, Vashi
' x='0' y='0' height='100%25' width='100%25' xlink%3Ahref='data%3Aimage/jpeg;base64,/9j/4AAQSkZJRgABAQAAAQABAAD/2wBDABALDA4MChAODQ4SERATGCgaGBYWGDEjJR0oOjM9PDkzODdASFxOQERXRTc4UG1RV19iZ2hnPk1xeXBkeFxlZ2P/2wBDARESEhgVGC8aGi9jQjhCY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2NjY2P/wAARCAAFAAoDASIAAhEBAxEB/8QAFgABAQEAAAAAAAAAAAAAAAAAAAMG/8QAGRAAAgMBAAAAAAAAAAAAAAAAAAECERIh/8QAFAEBAAAAAAAAAAAAAAAAAAAAAf/EABQRAQAAAAAAAAAAAAAAAAAAAAD/2gAMAwEAAhEDEQA/AMlqKjWVUl0iABf/2Q=='%3E%3C/image%3E%3C/svg%3E)

It has been a while now since the COVID-19 pandemic, and people are slowly learning of many different ways to deal with it — both in terms of recovery and prevention. It is a known fact that the virus, once it is inside the body, does not isolate and attack the respiratory system alone, but instead makes its way to many other organs.
Dr Md Shakeel, Head-Emergency & Trauma, Hiranandani Hospital, Vashi — a Fortis Network Hospital — says a study conducted in Italy showed that 87.4 per cent of patients, who had recovered from COVID-19, reportedly felt some kind of fatigue and dyspnoea (laboured breathing). This was reported even after two months of being discharged from the hospital.
“Some patients who had recovered had to be rushed back with low oxygen saturation levels, just a day after discharge. These patients were admitted to the hospital for at least 10 more days, and were discharged only after they started doing well. These patients returned to the hospital with a whole spectrum of lung diseases – from fibrosis (formation of hard fibrous tissues as the lung heals from an injury) to secondary infections and pneumonia. It was also noted that after recovering from COVID-19, some patients came back with reduced heart function, heart attack or even stroke,” he says.
ALSO READ | Home-based care for COVID-19 infection; here are some dos and don’ts
Dr Shakeel goes on to say that the virus — which is known to attack the endothelial cells that line the blood vessels — causes excessive blood clotting in the body. And now that the infection has been in the country for over five months, we need to start looking at post-COVID-19 rehabilitation.
“These long and short-term impacts are called ‘post-COVID syndrome’. This means, after the acute phase of COVID-19 is over, patients come back to hospitals with symptoms such as lethargy, body aches and itchy throats, even four to six weeks later. Patients are also seen to have had some psychological stress, leading to anxiety and depression. It is of utmost importance to monitor such cases, and a proper post-discharge rehabilitation plan be put in place, to monitor the patient’s health, so timely intervention can be done,” he explain
The doctor says that there are some things that COVID survivors should assess:
* Their daily check of oxygen saturation, it should be maintained at >94% in room air.
* They must watch for respiratory symptoms like persistence or worsening of cough and breathlessness.
* Check for persistent rise of body temperature above 100F.
* Watch out for signs of lethargy, drowsiness, and altered sensorium.
* Regular monitoring of blood sugar in known diabetic patients. COVID infection (as any other infection) alters blood sugar levels of the body. Strict monitoring once in three days and regular consultation with your doctor is required.
* Regular blood pressure monitoring in known hypertensive patients is required to avoid accelerated hypertension-related complications. Weekly blood pressure monitoring in case of controlled hypertension, or more frequently in case of abnormal readings, is required.
* Follow up consultation with the doctor within seven days of discharge.
* Blood investigations like CBC, CRP at first follow up, and subsequent follow-ups, if advised by a physician.
* Repeat CT scan of chest after three months to look at the extent of lung recovery post-infection.
35YR/M WITH VIRAL PNEUMONIA SECONDARY TO COVID 19 INFECTION

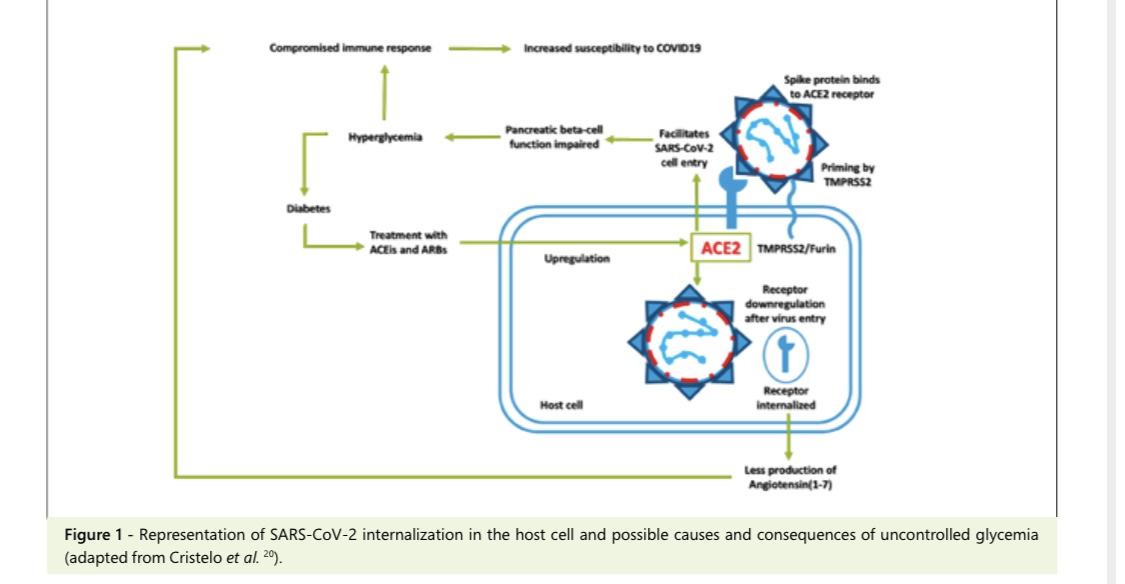
New onset of DM in Covid-19:
- Similar to SARS-CoV which caused an epidemic in 2002- 03, the novel coronavirus enters cell hosts through Angiotensin II Converting Enzyme receptor (ACE2). This receptor is found throughout the body and its pulmonary distribution explains, not only the respiratory clinical features, but also the acute respiratory distress syndrome that leads to severity of the disease.
- ACE2 receptor is found in the pancreas, both on exocrine cells and in the endocrine cells, that constitute pancreatic islets. Interestingly, its expression is also relevant in the endothelial cells of the microvasculature supplying beta-cells that produce insulin.
- As it has been postulated, upon the 2003-SARS pandemic, coronavirus spike protein enters the cells using the ACE2 receptor, initiating an inflammatory response that leads to apoptosis. Previous studies attempting to understand the pathophysiology of the SARS-CoV-2 infection over different organs and systems, have su- ggested that, following viral entrance and cell infection, ACE2 receptor is downregulated in lung tissue, which subsequently may trigger an inflammatory response.
- Although SARS-CoV-2 could directly impair insulin production of beta-cells, diminishing its function and disturb glucose metabolism, would that be enough to com- promise insulin production in a long-term manner and induce type 1 diabetes? Is there any immune mediated process? Or is ACE2 downregulation the factor at stake?
- One hypothesis could be that the cytokine storm - caused by the severe inflammatory response taking place in the lungs also targets the pancreas possibly causing diabetes .
- Other hypothesis is related to the role of the renin-angiotensin system (RAS) and its counterbalancing arm, the ACE2-Ang(1-7)-Mas axis on the development of diabetes. It has been shown previously how ACE2 decreased activity is detrimental for the development of acute respiratory distress syndrome (ARDS), verified both during the SARS-CoV epidemic as well during the current pandemic of COVID-19.
In recent years, it has also been proposed that stimulation of the ACE2-Ang(1-7)-Mas axis could be protective against deleterious effects of diabetic nephropathy, hypertension and diabetic retinopathy and that patients with diabetes have lower Angiotensin-(1-7) levels and lower activity of ACE2. These findings are consistent with the clinical features of patients infected by SARS- -CoV-2: that develop de novo hyperglycemia with difficult metabolic control, since there is downregulation of the ACE2 receptor which is internalized.
A 45 year old female with viral pneumonia secondary to Covid-19
A little difference that altered the entire covid recovery game: a report of two patients with focus on imaging findings .

42 YEARS FEMALE PATIENT WITH VIRAL PNEUMONIA SECONDARY TO COVID-19https://93deepanandikonda.blogspot.com/2021/05/42-years-female-patient-with-viral.html
58 years female patient with viral pneumonia secondary to covid-19


COVID with ICU psychosis
CvA
Family (and lack of visitation)
Clotting problems
Oxygenation issues
Virus itself
Immobilization
Drugs (eg, benzodiazepines)

A 42YR OLD MALE WITH FEVER AND COUGH.


A 62 YEAR OLD MALE PATIENT WITH FEVER , COUGH AND SHORTNESS OF BREATH

A 38 Y/O Male with Viral Pneumonia Secondary to COVID-19

A 48 year male with viral pneumonia due to COVID
A 65 YEAR OLD FEMALE WITH FEVER, SHORTNESS OF BREATH, DRY COUGH AND GENERALISED WEAKNESS

CASE DISCUSSION ON VIRAL PNEUMONIA SECONDARY TO COVID 19
o2 supplementation with 15 L/min
Neb with DUOLIN+BUDDCORT 6th hourly inj.
CPAP- continuous pasitive air pressure
Bipap
Mechanical ventilation




Comments
Post a Comment