Dengue fever with thrombocytopenia
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan
K.shirisha
Rollno;68
Chief complaints:
A 28 year old female staff nurse by occupation came to the casuality with complaints of
Fever since 4 days
Body pains since 4 days
Vomitings since yesterday night
Pain in lower abdomen since yesterday night
HISTORY OF PRESENT ILLNESS :
Patientwas apparently alright 4days ago
then she developed low grade fever, intermittent type which progressed to highgrade fever, continuous type since last night
Also associated with chills,
bodypains, Burning micturition and pain in lower Abdomen (since yesterday) dull aching type
H/O vomitings since yesterday night contained food particles,non bilious,non projectile associated with nausea.patient was referred from outside hospital to our hospital due to fever with thrombocytopenia (58,000)
No c/o hematmesis,melena, bleeding gums.
No h/o giddiness,
HISTORY OF PAST ILLNESS
No H/o Tb,asthma,Dm, Hypertension,CVA,cad,epilepsy
Surgeries: H/o 3 lscs 3 years back
2014-may 2
2017-oct 18
2020-feb 7
personal history:
Appetite decreased since 4 days
Diet: mixed
Bowel and bladder: regular
Sleep: adequate
No addictions
Family History:
Her father is a k/c/o DM2 since 7 years
Mother is a k/c/o hypertension since 3 years
General examination:
Patient is conscious coherent cooperative
Pallor: present
No icterus, cyanosis, clubbing, lymphadenopathy,edema

Vitals:
Temp: 100F


PR: 113bpm
RR: 18cpm
Bp:100/70 mmHg
Spo2:100% on Ra
Grbs:106 mg/dl
Systemic examination:
Cvs:
S1,S2 +, no murmurs
Rs: clear,Bae+
CNS: HMF+
Tone : normal in all limbs
Power: RT. LT
U/L. 5/5. 5/5
L/L. 5/5. 5/5
Reflexes:
B. T. S. K. A. P
R. ++. ++. ++. ++. ++. Flexion
L. ++. ++. ++. ++. ++. Flexion
P/A:


Auscultation:
Bowel sounds: heard
Diagnosis:
Dengue NS1 positive with thrombocytopenia
Investigations:
Hemogram:
D-1. D-2. D-3. D-4. D-5. D-6
HB. 15.5. 15 .6. 13.4. 12.5 13.4. 13.3. 13
TLC. 5,600. 5,600 6100. 4000 3900. 4200 2,900
PC. 58000 64000. 60,000. 49000 42000 45000 80000
I:. Ncnc thrombocytopenia
RBS: 89 mg/dl
16/1/23
HB: 14.1
TLC:5,600
PC:1.41 lakhs
RFT:
Blood urea: 48
Serum creatinine: 1.1
Na: 136
K: 3.4
Cl:100
ICA: 0.85
LFT:
TB: 0.90
DB:0.20
AST:66
ALT:31
ALP:205
TP:6.1
Albumin:3.18
A/G:1.09
Serology: negative
NS1 Antigen: positive
Cue:
Colour: pale yellow
Albumin : present +
Sugars: nil
Pus cells: 6-8
Epithelial cells:2-4
Chest x ray:

ECG:

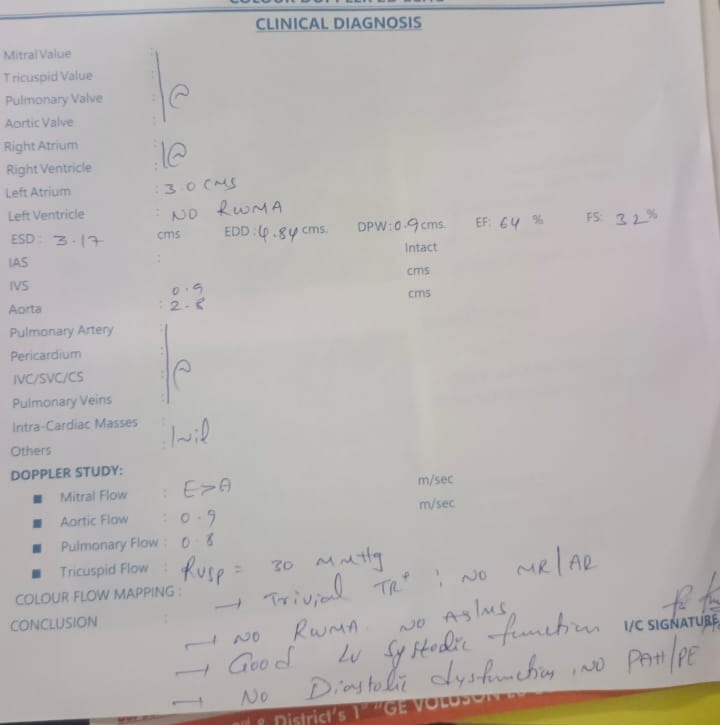
2d echo:
USG Abdomen:

Treatment:
IVF NS RL @ 75ml/hr
Inj Neomol 1 gm iv/sos if temp > 101 F
Tab Dolo 650 mg po/BD
Inj Zofer 4mg iv/bd
8am- 8pm
Inj pan 40mg /iv/od
8am
Grbs,pr,bp,temp monitering 4th hrly
13/1/23 Ward patient Unit 2 Dr.Aashitha sr Dr .manasa pgy3 Dr. Hari priya , pgy2 Dr. Lohith pgy1 Dr Nithin pgy1 Dr.shirisha intern Dr.vishal intern Dr.preethi intern S: ℅ dry cough pain abdomen,tightness of abdomen Stools passed O: Patient was conscious ,coherent, cooperative Vitals: Temperature: afebrile 98.7f Bp: 110/70 mmHg supine 110/80 mmHg standing HR: 78 BPM supine 88bpm standing RR:20cpm P/A: soft ,distended Tenderness present in epigastrium and hypogastrium No guarding rigidity Bowel sounds: heared Cvs: S1,S2+, no murmurs CNS: No focal neurological deficit RS: clear,BAE+ A: Viral pyrexia with thrombocytopenia Dengue NS1 positive P: IVF NS RL @ 100ml/hr Inj Neomol 1 gm iv/sos if temp > 101 F Tab Dolo 650 mg po/BD Inj Zofer 4mg iv/bd 8am- 8pm Inj pan 40mg /iv/od 8am Tepid sponging Grbs,pr,bp,temp monitering 4th hrly
14/1/23 Ward patient Unit 2 Dr.Aashitha sr Dr .manasa pgy3 Dr. Hari priya , pgy2 Dr. Lohith pgy1 Dr Nithin pgy1 Dr.shirisha intern Dr.vishal intern Dr.preethi intern S: ℅ dry cough (relieved) pain abdomen,tightness of abdomen( relieved) No fever spikes Stools passed O: Patient was conscious ,coherent, cooperative Vitals: Temperature: afebrile 98.7f Bp: 100/70 mmHg supine 90/70 mmHg standing HR: 78 BPM supine 88bpm standing RR:20cpm P/A: soft ,distended Non Tender No guarding rigidity Bowel sounds: heared Cvs: S1,S2+, no murmurs CNS: No focal neurological deficit RS: clear,BAE+ A: Dengue NS1 positive with thrombocytopenia P: IVF NS RL @ 100ml/hr Inj Neomol 1 gm iv/sos if temp > 101 F Tab Dolo 650 mg po/sos Inj Zofer 4mg iv/sos Inj pan 40mg /iv/od 8am Tepid sponging Grbs,pr,bp,temp monitering 4th hrly
16/1/23
:
Loose stools since yesterday ( 5-7 episodes)
2 episodes since morning( resolved)
Tightness of abdomen ( decreasing)
No fever spikes
O:
Patient was conscious ,coherent, cooperative
Vitals:
Temperature: afebrile 98.7f
Bp: 120/80mmHg supine
110/80 mmHg standing
HR: 78 BPM supine
88bpm standing
RR:18cpm
P/A: soft ,distended
Non Tender
No guarding rigidity
Bowel sounds: heared
Cvs: S1,S2+, no murmurs
CNS: No focal neurological deficit
RS: clear,BAE+
A:
Dengue NS1 positive with thrombocytopenia
P:
IVF NS RL @ 100ml/hr
Inj Neomol 1 gm iv/sos if temp > 101 F
Tab Dolo 650 mg po/sos
Inj Zofer 4mg iv/sos
Inj pan 40mg /iv/od
8am
Tepid sponging
Grbs,pr,bp,temp monitering 4th hrly
Course in hospital A 28 years old female came with history of fever and generalised weakness,on routine investigations was found to be Dengue NS1 positive and further management has been done based on the hydration status and platelet counts and no history of giddiness,loose stools ,significant postural hypotension and bleeding manifestations,and her platelets trends being,
On day-1: 58,000
On day-2: 64,000
On day-3: 60,000
On day-4: 48,000
On day-5: 45,000
On day-6: 80,000
On day-7:1.4 lakhs
No SDP transfusions were done,and the patient is being discharged as the vitals are stable and patient is relieved,and platelet counts are increased.
Question
Why thrombocytopenia is a common in dengue infection
Thrombocytopenia is a common laboratory finding in dengue infection. It usually reaches its nadir during the critical phase and resolves subsequently. The pathophysiology of thrombocytopenia in dengue infection is not clearly understood. It is believed that it rests mainly on two events:
1)decreased in bone marrow production and/or2) increased peripheral destruction and clearance of platelets.
Immune-mediated clearance of antibody-coated platelets has been proposed as one of the mechanisms leading to thrombocytopenia. The cross-reactivity of antibodies directed against NS-1 antigen and platelets suggests the role of antiplatelet antibody in the pathogenesis of thrombocytopenia.In addition, complement-mediated platelets destruction plays an important role during dengue infection.
Why polyserositis is seen in dengue?
Most critical future in dengue remains the leakege of plasma .This leakage of plasma is due to increased endothelial capillary permeability.This may present as ascites,pleural effusion,pedal edema and hemoconcentration.
Conclusion:
The reported women with Dengue fever with thrombocytopenia have been managed by fluids correction based on her hydration status to maintain sufficient urinary output and perfusion
In the above patient poly serositis is due to dengue fever leading to increased endothelial permeability And plasma leakage
Serositis is the predictor of impending dengue shock syndrome and was treated successfully with fluid replacement therapy.
Once dengue shock syndrome was treated serositis resolves on its own .



Comments
Post a Comment